What type of incision should you get for your Breast augmentation procedure? In addition to the implant size this is another very important decision that you need to make.
It seems to me when I ask a patient whether they have a preference as to what kind of breast incision they want, the most common answer is that they want the type of incision that they have seen on a friend.
Likewise, the second most common comment is “I don’t want such and such incision because somebody I know had one and it looks bad”. The truth is every type of incision has its pros and cons. Here is my explanation of the types of Breast augmentation incisions:
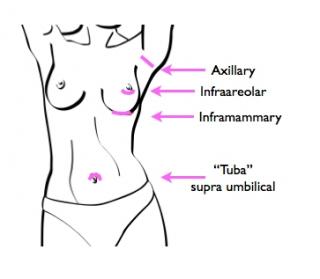
The inframammary incision
This is the incision I learned in my plastic surgery residency (20++ years ago!). It is also the most commonly used nationwide. This incision is placed under the breast along the fold. The advantages are that it is technically easy to perform, and it is well hidden under the breast.
The disadvantages are that once in a while, if the implant settles down on the chest wall, the scar will be visible in the bottom pole of the breast. It can also be a troublesome scar if it hyperpigments (gets darker colored), because then it is very visible. It can also hypertrophy(get thick), in which case it can be hard to treat and may need revision.
I use it mainly for large silicone implants, or if I think I’m going to have trouble fitting the implant through the infra areolar incision.
The infra areolar incision
This is the Breast augmentation incision I use most commonly. This incision is placed in the bottom half of the nipple perimeter. Most patients are concerned because it is in a visible place, and they are worried about loss of nipple sensation.
It has been my experience that although the scar is in a visible place it does fade very well. When I take long term (over 1 year) follow up photographs, I stand at 4-6 feet from the patient, and most times I have to ask what kind of scar they had, because I can’t see it. As far as loss of sensation, it can occur with any incision, and it has to do with a nerve that comes from the side of the chest wall and goes to the nipple. It is a very rare event, but unrelated to the type of incision.
The axillary incision
The axillary incision is ideal when you want no scar in the breast. The axillary incision is made in the armpits. It is close enough to the breast where you can get an instrument and see what’s going on inside. It is best suited for breasts that have little or no ptosis (drooping). If the breast hangs a little or it has a constricted base, I prefer the infraareolar or inframammary incision because it is nearer to the area I’m working on.
Some patients complain of pain in the axillary incision, but this is usually a temporary issue. The scar can hypertrophy in the postoperative period, but after a while it is almost invisible in the armpit.
Like the infra areolar incision, it can be hard to put a larger silicon implant through the axilla. In some cases, the placement of the implants can be a smidge high, but this is less of a problem for the experienced surgeon.
The TUBA – TransUmbilical Breast Augmentation
The TUBA incision location is thru the belly button. I don’t use this incision. Neither do most plastic surgeons. Many have tried it and abandoned it. A few plastic surgeons have become very proficient at it and love it.
Its main virtue is that like the axillary scar, it’s not in the breast. Its main problem is that it’s kind of far from the breast. There’s just not the same degree of control of the pocket that one gets with direct vision of the pocket. It is best suited for saline implants.
Like the inframammary scar, when it’s bad, its really problematic. Still, some patients really love it. I like the idea of it, but I’m doing so many silicon implants, its not very applicable to my practice.
Summary- there is not one best breast augmentation incision
In summary, there is not one best incision for Breast augmentation. Even though I have my favorites, I know that every case is individualized. The best approach for any given patient comes from a discussion of pros and cons of each approach with the surgeon. Be sure to ask your plastic surgeon what your choices are! You deserve the right to know.
(originally published on November 14, 2008)



{kind=link}
Zulema L. Stroop says:
Dr. Ricardo L Rodriguez says: